Knee recurvatum, or genu recurvatum, is a deformity of the knee characterized by hyperextension of the knee in the weight-bearing phase of gait. It is a walking impairment frequently observed in adult neurological rehabilitation – particularly after stroke, hemiparesis or congenital malformation. Visible to the naked eye, this phenomenon is not a pathology in itself, but an exaggerated extension of the knee which reveals an underlying cause that it is essential to identify in order to propose an effective correction strategy.
In this article, we review 8 causes of knee recurvatum, based on 22 years of clinical experience in neurology.

What is genu recurvatum?
During the stance phase of the step, instead of remaining slightly flexed, the knee locks into hyperextension. This attitude may be forced (physical effect) or adopted voluntarily (useful compensation). Genu recurvatum is often a multifactorial symptom.
How do you recognize a recurvatum knee and what are the symptoms?
Knee recurvatum is manifested by the following signs:
- Knee hyperextended during stance phase (knee “snaps” back)
- Asymmetrical gait and lameness
- Sensation of knee instability or locking
- Long-term ligament pain in cases of associated ligament laxity
- Increased fatigue on walking
This deformity can be observed in a static standing position or only during dynamic walking, depending on the origin of the disorder.
What causes knee recurvatum?
There are two main categories: mechanical causes (biomechanical constraints) and functional causes (compensations adopted by the patient).
| Mechanical causes (physical effect) | Functional causes (useful compensation) |
| 1. Limitation of ankle dorsal flexion | 5. Cerebellar Syndrome |
| 2. Quadriceps Hypertonia | 6. Weakness of Knee Extensors |
| 3. Hamstring Weakness | 7. Pain in forefoot |
| 4. Foot Dorsiflexor Deficit | 8. Fear of Knee Failure |
4 mechanical causes of recurvatum: understanding the physical effect
These first mechanical causes correspond to biomechanical constraints that force the knee to hyper-extend to allow progression. They are directly linked to knee deformity or musculo-articular dysfunction.
1. Limitation of Ankle Dorsiflexion
- Possible causes: hypertonia of triceps sural, muscle stiffness, tendon retraction, joint limitation (e.g. arthrodesis).
- Consequence: the leg cannot move forward correctly over the foot in the standing position, the knee moves backwards (limiting the pivot on the ankle).
2. Quadriceps Hypertonia
- The knee extensor muscle pushes excessively on extension, creating an exaggerated extension of the lower limb.
- This hypertonia is common after stroke or in spastic hemiparesis.
3. Hamstring Weakness
- The flexor muscles no longer sufficiently restrain knee extension during loading (to prevent hyperextension).
- Imbalance between quadriceps and hamstrings encourages recurvatum, particularly in cases of advanced knee osteoarthritis or neurological sequelae.
4. Foot Dorsiflexor Deficit
- The action of the foot lifter allows the tibia and knee to anteriorize at the start of the stance phase.
- Its deficit, often observed after a congenital malformation or neurological lesion, disrupts the mechanics of progression.
4 functional causes of recurvatum: the body’s compensations
In these cases, hyperextension is a functional strategy – a useful compensation – adopted by the patient to secure support despite an underlying deficit.
5. Cerebellar Syndrome
- To limit degrees of freedom and stabilize the leg, the patient voluntarily locks their knee.
- This strategy compensates for the lack of coordination and dynamic balance characteristic of cerebellar damage.
6. Weakness of Knee Extensors
- The recurvatum “locks” the knee without muscular effort, ensuring stable support despite quadricipital weakness.
- This compensation is useful in the short term, but deleterious to ligament structures in the long term (risk of ligament laxity).
7. Pain in forefoot
- The patient avoids anterior support and places himself in posterior support, favoring recoil of the knee.
- This functional cause is often underestimated when analyzing the causes of recurvatum.
8. Fear of Knee Failure
- For fear of falling, the patient locks the knee in hyperextension to secure the stance phase, even if the force is normal.
- The psychological component plays a major role in the functional causes of post-stroke recurvatum.
How to treat knee recurvatum: treatment and rehabilitation
Recurvatum treatment must be tailored to the identified cause. Here are the main therapeutic approaches:
Active rehabilitation and therapeutic exercises
Active rehabilitation is at the heart of the treatment. Here are 3 practical therapeutic exercises:
- Ankle mobility work: stretch the sural triceps while standing against a wall (3 × 30 sec), to restore dorsal flexion and limit knee compensation.
- Eccentric hamstring strengthening: from a standing position on one leg, control the descent slowly (3 × 10 repetitions), to regain control of the extension.
- Proprioceptive work in monopodal support: on an unstable platform, hold the knee slightly bent (3 × 30 sec), to rebuild joint awareness as a basic therapeutic exercise.
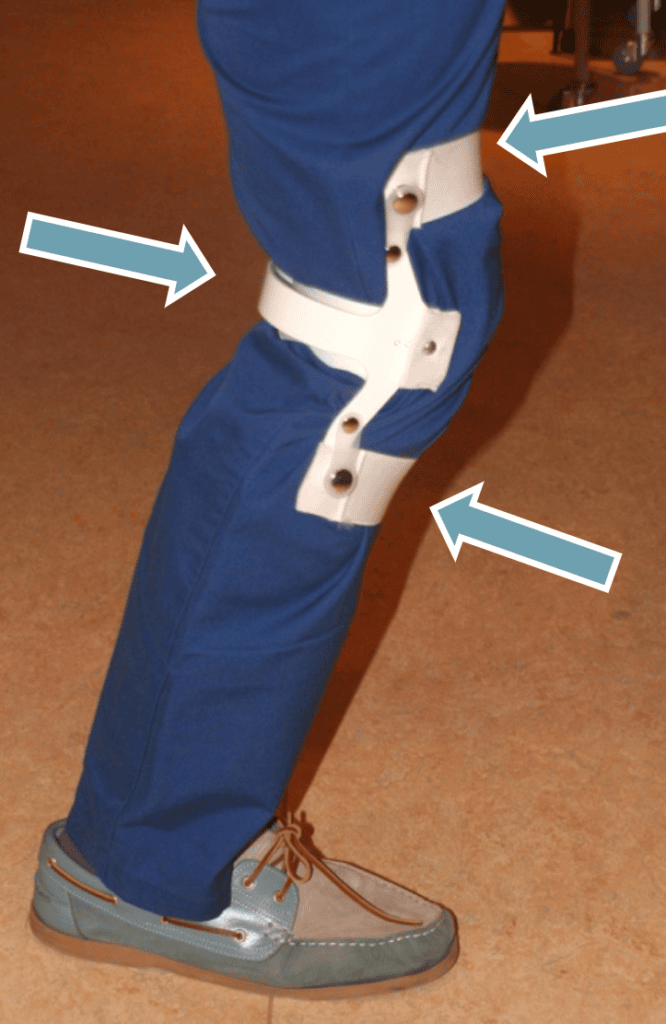
Orthotics
The anti-recurvatum knee brace is a valuable tool for mechanically limiting hyperextension. It secures walking while enabling rehabilitation. It is particularly indicated in the first few weeks post-stroke, or in cases of significant ligament laxity, to stabilize and protect the joint.
Anti-equinus orthotics are also invaluable, as they act on one of the main causes of recurvatum: the equinus of the foot.
Adapted technical aids
Technical aids such as the Wheeleo® help you to progress more smoothly and symmetrically, by limiting certain inappropriate compensations and facilitating postural and proprioceptive correction.
Treatment of spasticity
Treatment with botulinum toxin injections and neurotomy improves recurvatum.
Is genu recurvatum curable? Prognosis and outlook
Prognosis depends directly on the cause identified. Genu recurvatum of functional origin (compensation) can often be improved by active rehabilitation. Purely mechanical forms may require longer treatment, or even surgery in cases of bone deformity or severe ligament laxity. Causes related to hemiparesis or stroke have a variable recovery potential, depending on the extent of brain damage.
Why identifying the cause of recurvatum is essential
Understanding the cause of recurvatum makes it possible to choose a targeted therapeutic approach to relieve recurvatum and identify the precise cause :
- Joint mobility work (ankle, knee)
- Muscle strengthening (ischios, quadriceps) through active rehabilitation
- Gait pattern education
- Postural and proprioceptive correction
- Knee orthosis adapted if necessary
- Surgical or drug treatment (botulinum toxin, neurotomy, tenotomy, etc.)
- Adapted technical aids such as the Wheeleo®.

Conclusion
Knee recurvatum is never trivial: it reflects an imbalance that needs to be carefully analyzed. Whether it’s the consequence of a deficit, hypertonia or an adaptation strategy, it’s essential to understand the cause in order to better support the patient towards a more functional and secure gait. Whether it’s a post-stroke case with hemiparesis, a congenital malformation, or simple mechanical compensation, each case deserves an individualized assessment.
What about you? What causes recurvatum have you encountered in your practice?
